

Why it happens
Topics on this page:
What causes Abnormal Uterine Bleeding?
Understanding what causes abnormal uterine bleeding will help to give you answers about why your period has changed, or has always been difficult.
Abnormal uterine bleeding may be due to structural or non-structural causes.
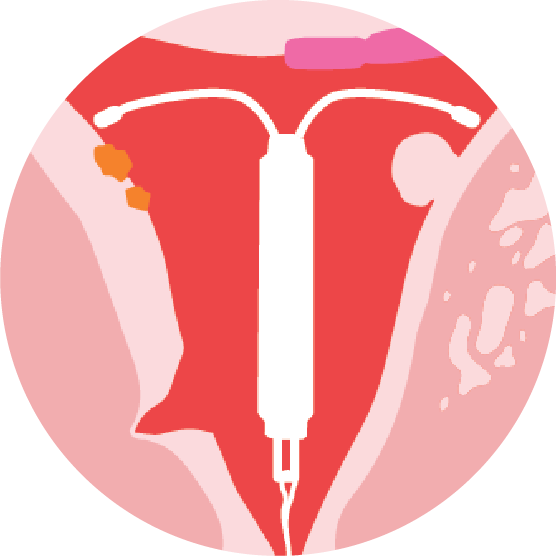
Structural causes refer to things that change the structure of your uterus, like polyps or fibroids and you can see these in the picture below. These can be suspected on history taken - using questions regarding your menstrual cycles or periods. And they may be observed at the time of examination of your tummy or through the vagina, using imaging (such as ultrasound) or a procedure (such as hysteroscopy).
Non-structural causes refer to anything that can't be seen by physical examination or imaging. These include hormonal imbalance, clot disorders (bleeding dysfunction), and medication side effects, among others.
The acronym PALM-COEIN has been developed over many years by doctors and researchers to help develop an international standard to describe the causes of AUB. Each letter represents a different cause - the structural causes are represented by the acronym PALM and the non-structural causes by COEIN.
PALM-COEIN
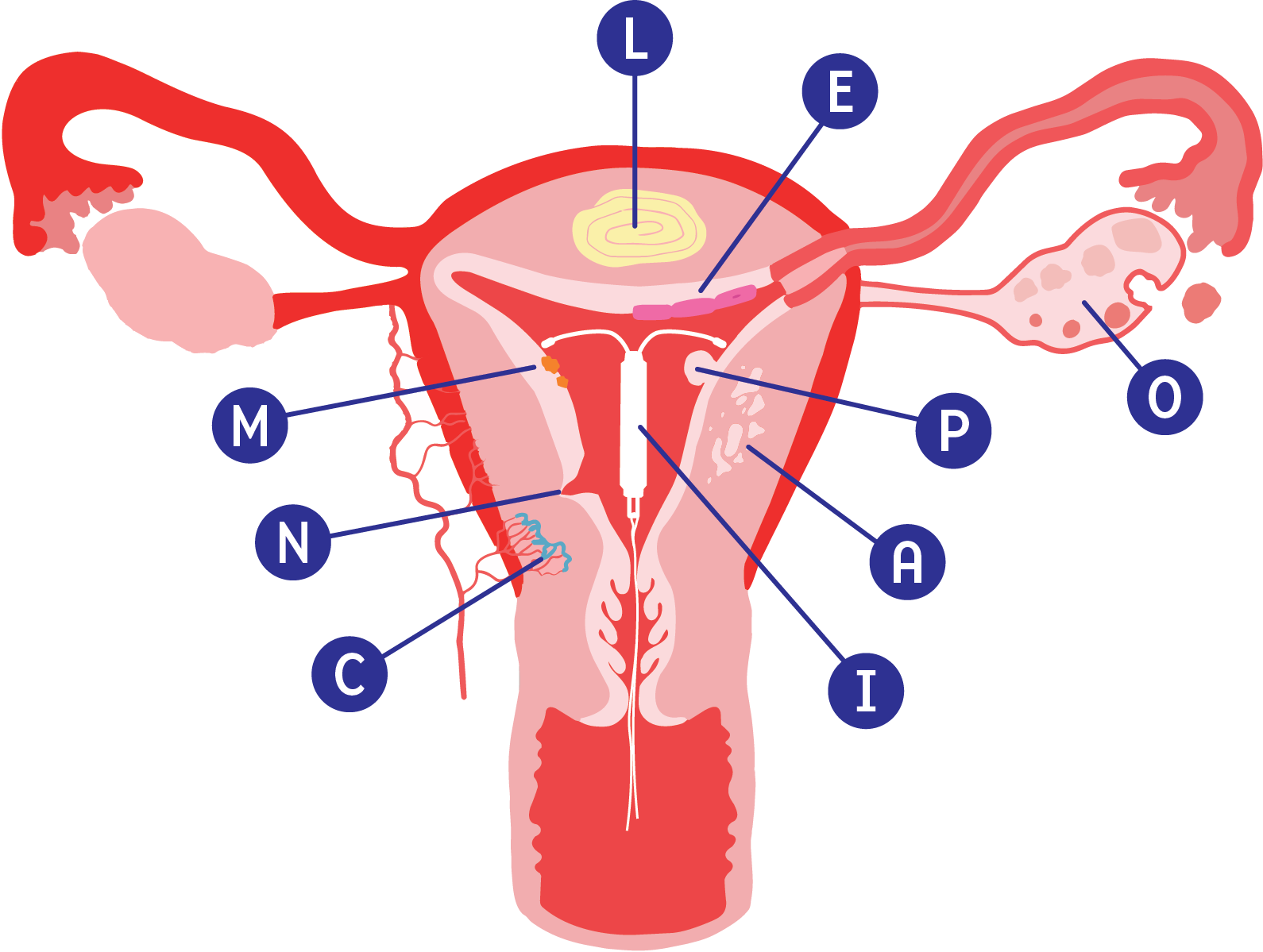
Structual causes
P - Polyp
A - Adenomyosis
L - Leiomyoma
M - Malignancy
Non-structual causes
C - Coagulopathy
O - Ovarian dysfunction
E - Endometrium
I - Iatrogenic
N - Not otherwise classified
Structural causes

P - Polyp
Can arise from the inner lining of the uterus (endometrium), the neck of the womb (cervix) or both. The tissue grows or expands in a specific area (focal overgrowth) and may grow into the inner part of the womb (uterine cavity) or into the cervix. According to their position, they are may be in the lining of the uterus (endometrial polyps) or in the cervix (cervical polyps). Polyps could cause irregular menstrual bleeding or bleeding after sex (post-coital bleeding). Most polyps are non-cancerous (benign).
A - Adenomyosis
The tissue from the inner lining of the uterus (endometrium) grows into the muscular wall of the womb (uterus). The displaced tissue continues to act normally — thickening, breaking down and bleeding — during each menstrual cycle, the most common symptoms are heavy menstrual bleeding and pelvic pain.

L - Leiomyoma
They are also called myomas or uterine fibroids. They are non-cancerous (benign) growths that develop from the muscle tissue of the uterus. They vary in size and position. They may bulge into the uterine cavity (submucosal fibroids), grow within the muscular wall (intramural) of the uterus, or form on the outer layer of the uterus (subserosal fibroids).
M - Malignancy or Hyperplasia
Cancerous growth in the inner lining of the uterus (endometrial cancer), the muscle wall (uterine sarcomas), or the cervix (cervical cancer). Hyperplasia refers to abnormal growth of the lining of the womb. These are a continuum of changes that could lead to cancer development. Different types of hyperplasia are associated with different risk.
Non-structural causes
C - Coagulopathy
A condition in which the blood's ability to form clots (coagulate) is impaired. It is also called a bleeding disorder, and may lead to AUB.

O - Ovarian dysfunction
Changes in normal functioning of ovaries resulting in hormonal imbalance. It can occur as part of normal body function (adolescence, perimenopause, breast feeding, pregnancy),due to a disease (such as, but not limited to polycystic ovarian syndrome-PCOS, thyroid disease, extreme body weights, pituitary gland dysfunction) or other factors such as extreme exercise.

E - Endometrium
This is considered to be due to abnormal function of the endometrium, there is very limited information about this.

I - Iatrogenic
Medical treatment-related causes such as the use of hormonal treatments (such as contraceptives), or blood thinners.
N - Not otherwise classified
Group of causes that do not fit in any of the previous categories. For example, caesarean scar defect or chronic inflammation of the endometrium.
Other topics related to abnormal uterine bleeding and pain
Endometriosis
Endometriosis itself does not cause the uterus to bleed abnormally. However, endometriosis can indirectly cause abnormal bleeding by impacting the ovaries. Heavy menstrual bleeding may be a symptom of endometriosis if associated with other symptoms.
See Endometriosis New Zealand: https://nzendo.org.nz/
https://ranzcog.edu.au/wp-content/uploads/2022/06/Endometriosis_pamphlet.pdf
Menopause
The “menopause’’ is determined after a year has passed after your last period, and due to the natural end of your ovaries' cyclical hormonal production. It is usually experienced around 50 years of age, or if both ovaries have been surgically removed. Perimenopause is the time leading up to the last menstrual period and one year after the last period. It is common to have irregular periods and symptoms such as hot flushes, night sweats, muscle and joint aches and breast tenderness. If the symptoms are impacting your life or you have heavy bleeding, you can seek medical help.
For more information, see https://ranzcog.edu.au/wp-content/uploads/2022/06/Menopause-pamphlet.pdf
https://info.health.nz/health-topics/conditions-treatments/womens-health/menopause
Post menopausal bleeding (PMB)
Post menopausal bleeding (PMB) is defined as bleeding after the acknowledged menopause. Post menopausal bleeding is always abnormal. It is important to always seek medical advice if you have post-menopausal bleeding.
It is common and can range from spotting (a pink or brown discharge) to heavier period-like bleeding. The cause can be thinning of the walls of vagina or the lining of the uterus (vaginal atrophy), thickening of the lining of uterus (hyperplasia) often due to menopause hormone therapy (MHT) or cervical polyps. About 1 in every 10 people, bleeding after menopause is caused by cancer of the uterus or cervical cancer. Treatment depends on the cause of bleeding. It may include local oestrogen cream for vaginal dryness, removal of cervical polyps, hormonal and surgical treatments for endometrial hyperplasia or cancer treatment.
For more information: https://info.health.nz/health-topics/conditions-treatments/womens-health/menopause/bleeding-after-menopause
Painful periods (dysmenorrhea) and chronic pelvic pain
Dysmenorrhea is the medical term for painful periods. Some mild pain or discomfort with your periods may be normal. For some people, the pain keeps them from doing their normal activities, which is not normal. If this is your experience, you should consider seeing your doctor and get help. Severe pain may also be accompanied by nausea, vomiting, diarrhoea, low back pain, migraines, dizziness, fatigue, insomnia, and sometimes, fainting or passing out.
Chronic pelvic pain is defined as pelvic pain that lasts longer than 6 months. Pain can come and go or be constant, and can also occur during or outside your period. Chronic pelvic pain may have different causes, and if this is your experience, you should consider seeing your doctor. Chronic pelvic pain may be related to some causes of abnormal uterine bleeding, but it is not always explained by a structural cause that could be surgically removed.
Pain management
There is a range of different pain management strategies. These could include heat packs, pain medication (analgesics), physiotherapy and/or hormonal therapy to control or stop your periods (if the pain is associated with your periods). Some people have found benefits from counselling, mindfulness or changing their diet (may help reduce inflammation and-or pain).
You can also ask your doctor about pain management services in your region.
For more information: https://healthify.nz/health-a-z/d/dysmenorrhoea/
https://www.pelvicpain.org.au/for-women/
https://ranzcog.edu.au/wp-content/uploads/2022/06/Chronic-pelvic-pain.pdf